Prostatitis and Benign Prostatic Hypertrophy
Causes, Treatment and Prevention
|
Disorders
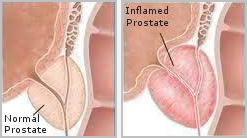
Many practitioners and patients seem to think that Zinc is a cure-all for all prostate-related problems, or that they all result from insufficient zinc intake, however only an enlarged prostate (Benign Prostatic Hyperplasia), or BPH, is at times linked to below-normal levels of zinc. Subsequently, with some exceptions, nutritional supplements used in the treatment of BPH will generally not work for Prostatitis, or may have to be avoided.
Prostatitis presents with above-normal, to typically very high cellular levels of zinc, and symptoms are invariably worsened by either supplementing extra zinc, consuming foods that are high in zinc, or by any other remedial aspect or dietary lifestyle that synergistically promotes greater zinc retention.
Some individuals claim that their condition improved after supplementing zinc, but it always turns out that they either did not have Prostatitis in the first place - i.e. they self-diagnosed their condition, or they were misdiagnosed by an unqualified practitioner.
However, even qualified urologists frequently disagree on the proper classification of the disorder and/or the best course of treatment, unless a patient presents with a conclusive, lab supported case of acute bacterial Prostatitis. The reason is simply that the term "Prostatitis" over the years has become synonymous with a variety of symptoms that include bacterial and non-bacterial Prostatitis, chronic pelvic pain syndrome, proctalgia (rectal pain), pudendal nerve entrapment, interstitial cystitis, and also Benign Prostatic Hypertrophy / BPH, for which zinc supplementation may actually be indicated and beneficial.
Commonly agreed upon causes of Bacterial Prostatitis include pathogens such as escherichia coli (E. coli), found in about 90% of patients, or proteus, enterobacter, pseudomonas, streptococcus and staphylococcus, serratia, untreated yeast infections and STDs (sexually transmitted diseases), and there are additional considerations of tuberculosis (tuberculous prostatitis), and other viral or bacterial infections. However it is agreed, that better than 90% of chronic prostate complaints are related to Non-Bacterial Prostatitis (with negative laboratory findings, or no documented culture), for which antibiotic treatments are not effective or indicated, and where generally no particular cause is found.
While it is recognized that Prostatitis can generate Referred Pain (usually in the lower back), it may also cause dental pain in the left upper or lower incisors, which coincides with flare-ups of Prostatitis. In turn, all incisors are equally capable of triggering chronic Genitourinary Pain.
The left 1st + 2nd upper or lower incisors are prostate / uterine-specific, and the right 1st + 2nd upper or lower incisors are bladder-specific, having the potential of causing chronic Prostatitis (left side), or interstitial or chronic cystitis (right side). In a couple of patients Dr. Ronald Roth had been able to trace the cause to failed root canal work, where their symptoms promptly and permanently disappeared following additional endodontic intervention, with no other treatments or remedies required.
It is not unusual for some men to experience left-sided Sciatic Pain in addition to prostate pain and burning, since most cases of non-surgical sciatica involve a zinc / potassium ratio conflict. Correcting the patient's zinc / potassium ratio will not only resolve sciatic pain, but any related prostate pain as well, provided zinc levels are normal. This can be accomplished through nutritional intervention (supplements, or some natural remedies), chiropractic adjustments, or through needle, or needle-less electro-Acupuncture.
In some cases, stomach acid-lowering medications appear to help improve Prostatitis symptoms, which is likely due to the calcium-retaining effect that many of these types of stomach remedies exhibit. Calcium is not only a very potent zinc antagonist, but it has significant anti-inflammatory properties as well. When taking larger amounts of calcium, it may be prudent to include higher doses of Vitamin D for its (prostate) cancer-protective properties also.
Since mainstream medicine does not have a very good track record in the successful treatment of Chronic Prostatitis (CP) - particularly abacterial varieties, many men look into Alternative Treatment Methods, - including natural home remedies - trying to resolve their prostate problems, and they frequently end up using a shotgun approach by combining all the advice gathered from various sources.
Herbal / Nutritional Remedies for Prostatitis
Remedies commonly recommended for prostatitis include Pygeum (from the bark of the African prune tree), Stinging Nettle, and Goldenseal. There are also a few anecdotal success stories involving the use of Cranberry Juice, or the flavonoid Quercetin. However, while adequate amounts of bioflavonoids (0 - 25 micromol/L) provide many health benefits, large amounts of quercetin (50 - 250 micromol/L), recommended by some advocates for Prostatitis, have been found to induce cytotoxicity and DNA damage in a number of rat studies.
Dietary treatments include the avoidance of foods high in zinc (shellfish, herring, organ meats, wheat germ, soybeans, and some seeds and nuts), which for some men may be difficult to follow, so supplementing zinc antagonists (see further below), may be a more convenient approach. There are claims that alcohol, coffee, chocolate, and cola drinks have an adverse effect on Prostatitis as well.
Antibacterial remedies that have proven successful in the treatment of other inflammatory conditions may be a consideration for Prostatitis sufferers who have not had much luck with any other "natural" remedies. They include the regular intake of a higher dose of fresh or freeze-dried Garlic, Turmeric, Sulforaphane caps, Mastic gum, and Probiotic (friendly bacteria) supplements, however if any of these cause bowel / intestinal disturbances, they may very likely worsen Prostatitis as well.
The herb Saw Palmetto, or Phytosterols are routinely recommended for the symptomatic treatment of an Enlarged Prostate (BPH). While some practitioners recommend these for Prostatitis also, none of the patients Dr. Ronald Roth had treated for Prostatitis and who had tried either saw palmetto, beta-sitosterol, or other sterols and sterolins, had found them to be helpful for that condition.
Since saw palmetto possesses alpha-5-reductase inhibitory activity (either inhibiting the conversion of testosterone to dihydrotestosterone, or blocking some effects of testosterone), its use has also been recommended in the treatment of male-pattern hair loss.
While zinc is pro-inflammatory, Copper is anti-inflammatory and also a zinc antagonist, so for some of those suffering from Prostatitis, a higher intake of copper-rich foods, or short-term copper supplementation can be helpful. Unfortunately, a considerable percentage of the population suffers from copper overload, which would therefore prohibit additional copper intake for most Prostatitis patients.
Due to the paired association of Potassium and Zinc, high potassium-containing foods or beverages should also be avoided because of the pro-inflammatory effect of high potassium intake on the bladder, which often has a negative effect on the prostate as well. For instance, chronic and acute bladder infections (cystitis) necessitate a potassium-lowering approach, which will resolve most (non-structural) chronic, inflammatory bladder problems, while interstitial cystitis (IC) requires a potassium-raising approach.
B-Complex has a zinc and potassium-raising effect, so higher amounts should not be supplemented. However as mentioned above, this only applies to Prostatitis but not BPH, which may actually benefit from an increase of B-Complex vitamins, including potassium. (for details, see "Zinc / Potassium" and "B-Complex").
In contrast to testicular cancer, which presents with very high cellular zinc levels (left side) or very high cellular potassium levels (right side), Prostate Cancer is seen with both, excessive and deficient zinc levels, in addition to elevated phosphate levels, so maintaining a normal phosphorus and zinc status is important from a preventive aspect.
With testosterone being closely related to zinc metabolism, prostate cancer is also more prevalent with below normal free testosterone levels (more common), and above-normal free testosterone levels (less common), which necessitates a similar preventive approach of trying to maintain normal testosterone levels throughout one's lifetime, in addition to following general guidelines of inhibiting the aromatase enzyme to reduce estradiol.
Some practical, clinical considerations for the treatment of Prostatitis and BPH:
- Since there may be more than one possible cause, a detailed diary should be kept of one's daily food and beverage intake, along with other activities (prolonged sitting...), to isolate, and subsequently help eliminate all potential causes of either Chronic Prostatitis, occasional flare-ups of Prostatitis, and/or other prostate related problems, including symptoms accompanying an enlarged prostate (Benign Prostatic Hyperplasia).
- Lowering cellular Zinc Levels through diet or nutritional supplementation provides the most effective, safest, and cheapest treatment approach for the great majority of Chronic Prostatitis sufferers, with the most common zinc antagonists consisting of Vitamin C, Calcium + Vit D, Selenium, Folic Acid, Vitamin A, Vitamin B1, and at times Iron - but rarely Copper, which should be individually matched.
- If digestive problems (i.e. bowel disturbances) accompany flare-ups of Prostatitis, then avoidance of the dietary triggers that cause the bowel irritation may prevent episodes of prostatitis. Common bowel irritants include foods containing a high Oxalic Acid content (Swiss chard, rhubarb, spinach, beets / beet greens, or cocoa products), beans, pickles, citrus, dairy products (except butter), some nuts, seeds and grains, or they may result from the use of sweeteners such as Xylitol or sorbitol.
If probiotics improve bowel functions, they may be helpful for Prostatitis as well, however if they trigger intestinal problems - common in some of those suffering from a compromised immune system - they will also worsen Prostatitis. Likewise, a higher intake of berries (e.g. blueberries), or hot spices (curry, cayenne, black pepper) may have the same positive or negative effect on Prostatitis as they have on bowel functions. - Foods contaminated with pathogens such as E.coli, that may be present on greens or lettuce (even after careful washing), or in under-cooked meats, are a well-known trigger for Bacterial Prostatitis. If antibiotics have failed to improve the symptoms of Bacterial Prostatitis, a combination of cranberry juice or extract, and sulforaphane caps in the 2,000 mcg a day range may be an option following an initially higher dose of 10,000 - 20,000 mcg / day, until symptoms are brought under control.
The use of prostate and bacteria-specific Nosodes may be required in some resistant cases, which may only be available through a medical practitioner. [Nosodes are remedies that are made up of pathogens or diseased tissue of the same type as being treated, but are highly potentized to trigger an immune response].
- If left-sided sciatica accompanies prostate pain, providing relief for sciatica usually reduces prostate pain as well. While supplementing zinc alone would theoretically help left-sided sciatica, this does not always normalize a low zinc / high potassium ratio since increased zinc levels may boost potassium levels also, so instead, one needs to supplement Chelated Chromium (not Picolinate or GTF) in the 1000 - 3000 mcg range, since chromium supports zinc retention, while lowering potassium at the same time. This will correct a patient's zinc / potassium ratio, and with it any related spinal alignment problems. However, zinc may be added if its levels are well below normal and if the pain is not due to Prostatitis.
Needle acupuncture, or especially needle-less electro-acupuncture may also be a treatment consideration, which will simultaneously provide relief from sciatic and prostatic pain. 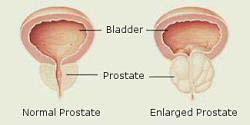 If nutritional remedies are used to treat an enlarged Prostate, then Chelated Zinc in the 10 mg - 100 mg range (depending on its deficiency) can be part of a formulation to help shrink the prostate, and may include Saw Palmetto, Ginseng, Vitamin A, Pumpkin Seed Oil, Nettle Root extract, Melatonin, Pygeum, among others.
If nutritional remedies are used to treat an enlarged Prostate, then Chelated Zinc in the 10 mg - 100 mg range (depending on its deficiency) can be part of a formulation to help shrink the prostate, and may include Saw Palmetto, Ginseng, Vitamin A, Pumpkin Seed Oil, Nettle Root extract, Melatonin, Pygeum, among others.
With the exception of Prostatitis, eating Pumpkin Seeds regularly provides all-round benefits for many urinary / prostate-related complaints, while many 'Cold' and 'Allergy' types-of medications have a reputation of worsening symptoms of an enlarged prostate.
Since a declining testosterone / estrogen ratio is a major factor in the development of BPH, a more simplified remedial approach - to reduce estradiol levels - consists of using 250 - 500 mg of Milk Thistle per day, along with zinc (if still required) and potassium, which will not only resolve the symptoms of an enlarged prostate, but reduce the risk of prostate cancer [1] as well.
• Chronic Prostatitis can develop secondary to suffering from ongoing bouts of Interstitial Cystitis, in which case - and unless interstitial cystitis is 'referred pain' related - a higher intake of supplemental potassium will resolve the interstitial cystitis, and any symptoms related to Prostatitis.
Since the average adult male requires close to 5,000 mg or more of potassium per day, the actual amount required through supplementation (to keep bladder / prostate-related symptoms under control), depends on a patient's androgen status (DHEA), whose decline with age reduces potassium retention (requiring higher intake), and they depend on how much potassium one gets from the diet.
A meal containing beans and potatoes may provide twice as much potassium as a meal consisting of rice and chicken, so supplemental requirements could range from a few hundred mg, to over a couple of thousand mg of potassium per day, depending also on other high-potassium sources consumed.
Excessive potassium intake may trigger symptoms ranging from frequent urination, to those of a bladder infection (cystitis), which unfortunately are also similar to those symptoms experienced with a low potassium status, except for a reduced volume of urine voided, and the potential of developing incontinence.
Just like acute, chronic, or interstitial cystitis go hand in hand with abnormally high, or abnormally low cellular levels of potassium (save for structural causes), Prostatitis and Benign Prostatic Hypertrophy go hand in hand with abnormally high cellular levels of zinc (prostatitis), and often below-normal cellular levels of zinc (BPH).
Instead, one can either follow a testosterone-boosting strategy to maintain normal zinc levels and use natural remedies such as Puncture Vine (tribulus terrestris), wild green Oats (avena sativa), Ginseng, Nettle Root, Muira Puama, or the flavonoid Chrysin (+ piperine, a pepper extract to help absorb chrysin), which will either boost testosterone levels, or reduce SHBG (sex hormone-binding globulin).
Or, as mentioned earlier, the treatment can simply consist of taking Milk Thistle to reduce estrogen (estradiol), which is frequently just as effective to successfully treat Benign Prostatic Hypertrophy, however with a history of prostatitis, only potassium - but not zinc - may be added if necessary.
It is also recommended to prevent exposure to other dietary or environmental sources of estrogen, such as hormone-raised meat products, or chemicals that mimic estrogen such as Bisphenol A, which are released when heating foods or beverages in some plastic containers.
- Low zinc levels - particularly post middle age or andropause - frequently go hand in hand with lower potassium levels, which can be a cause or contributing factor with Erectile Dysfunctions (impotence), and a host of cardiac, urinary, or hormonal / metabolic health problems, including weight gain. Regular intake of substances that negatively affect liver functions (Tylenol, alcohol, many prescription drugs...), can lead to the same consequences.
- Extra Zinc and/or Pantothenic Acid (Vitamin B5) in the 100 mg - 1000 mg range may help resolve the occasional presence of Blood in semen (hematospermia) if due to a low zinc / high phosphorus ratio.
Chronic bleeding from the Prostate is worsened by insufficient calcium intake (or a low Ca / Mg ratio), inadequate intake of bioflavonoids and Vitamin C, a high intake of remedies or spices with blood-thinning properties such as ginkgo biloba, fish oils, Vitamin E, garlic, turmeric, high oxalic acid sources, bromelain, alcohol, pomegranate juice, regular / high consumption of blueberries or juice, ginseng, and even larger and regular amounts of heart-healthy foods such as walnuts and fish. Saw Palmetto prolongs bleeding time, so it will worsen bleeding from the prostate also. A high Vitamin K intake will not counteract any of the above.
If side effects are not an issue (there is a rare breast cancer and high-grade prostate cancer risk), the drug Finasteride (Proscar) can be an effective treatment for bleeding from the prostate [2] by inhibiting the growth of small blood vessels within the prostate when due to Benign Prostatic Hypertrophy.
Drug-less intervention consisting of Milk Thistle + Potassium, or myrosinase enzyme-active Sulforaphane may also resolve chronic BPH-related blood in semen and chronic BPH-related bleeding from the prostate, provided there is no overuse of dietary, supplemental, or prescribed blood thinners. Clinical studies have shown that sulforaphane may also be effective in the prevention and treatment of BPH and prostate cancer.
- When starting out with normal zinc levels and a healthy prostate, and then - for whatever reason one begins to supplement high amounts of nutrients such as calcium, copper, selenium, Vitamin C, or folic acid, this will over time create below-normal levels of zinc (unless zinc is on the high side to begin with), which eventually will have negative implications on one's prostate.
The same situation applies in reverse. Even by supplementing an individually correct amount of zinc for an enlarged prostate (BPH), one still has to deal with the potential antagonism of zinc on any of the above mentioned nutrients (zinc antagonists), which over time may get depleted, and as a result may require extra supplementation as well. - Long-distance driving - or otherwise prolonged sitting - can trigger prostate pain or burning in men whose prostate has a tendency to swell, or has started to enlarge (usually post middle age), and where any undue pressure, including from constipation, irritates the prostate. Getting one's favorite home or work chair custom upholstered to create additional O or U-shaped padding on the seat will provide significant relief for many of these patients by reducing the pressure from the central part of the seat to the perineum, which also benefits those suffering from Pudendal Nerve Entrapment.
- Habitually holding one's urine is considered to be a possible contributing factor with Prostatitis by eventually damaging the prostate, with the theory being that in addition to humans, housebroken dogs seem to develop that condition as well.
- Empirical data suggests that frequent ejaculations are helpful to reduce flare-ups of Prostatitis, and a number of research studies found that they also help reduce the risk of prostate cancer.
From personal, clinical experience, lowering zinc levels through dietary or supplemental intervention has proven to be the most effective method to bring Prostatitis quickly under control, while an enlarged prostate (Benign Prostatic Hyperplasia) may benefit from extra zinc intake, however the control of its symptoms frequently requires the additional support of other prostate-specific remedies.
 Manganese may help with some symptoms of Parkinson's disease such as muscle rigidity and twitching...
Manganese may help with some symptoms of Parkinson's disease such as muscle rigidity and twitching...
 Research shows that phytosterols such as beta-sitosterol may help normalize the function of natural killer cells and T-helper lymphocytes...
Research shows that phytosterols such as beta-sitosterol may help normalize the function of natural killer cells and T-helper lymphocytes...
 Iron deficiency may be suspect with some forms of ADHD. 84% of children with ADHD were found to have abnormally low levels of ferritin...
Iron deficiency may be suspect with some forms of ADHD. 84% of children with ADHD were found to have abnormally low levels of ferritin...
 A high intake of B Vitamins can trigger heart palpitations, HBP, major complications in patients with congestive heart disease...
A high intake of B Vitamins can trigger heart palpitations, HBP, major complications in patients with congestive heart disease...