Iron and Manganese
| Cellular Nutrition
Iron (Fe) and Manganese (Mn) are associated trace elements considered essential to human health. As is the case with most other associated mineral pairs, the absorption of iron is dependent on manganese, however with manganese levels being frequently lower than iron levels, and with many forms of iron causing constipation or gastric upsets when supplemented, the addition of manganese, when low, is vitally important. This not only prevents further ratio conflicts between the two elements, but also substantially reduces the amount of iron needed when manganese is supplemented at the same time.
While some sources claim that manganese lowers iron levels, this is mostly a theoretical consideration that would only happen under unusual circumstances. In actual clinical settings, Dr. Ronald Roth had not seen a single case of a patient's iron (ferritin) levels decline as a result of taking manganese, even when doses as high as 150 mg per day were supplemented on an ongoing basis. In fact, most minor iron-deficiency situations can be dealt with by using manganese alone - without any iron - which reduces any potential adverse effects that can be part of routine iron supplementation.
In contrast to Acu-Cell Analysis, routine blood tests do not include manganese measurements, but use a number of iron determinations alone, none of which are very reliable to assess true iron requirements in a patient, with only ferritin levels being more useful, and being closer to actual intracellular values. As a result, patients are given far too many false positive and false negative recommendations (especially with polycythemia or thalassemia issues) to take - or not to take extra iron supplements, to the detriment of the patient.
Pregnant women are the most vulnerable targets for either insufficient, or excessive iron supplementation, with the latter being able to trigger 'Toxemia of Pregnancy' (high iron causes excessive sodium retention), and in which case higher amounts of Folic acid should have been supplemented instead, which lowers sodium
Likewise, blood loss, or malabsorption are considered to be the main causes for low iron after ruling out any of a number of blood disorders, however low iron can very easily result from manganese levels having been low for a long period of time, or from other factors such as excessive calcium, zinc, or magnesium levels reducing iron values. Cellular levels of iron best correspond to actual symptoms of excess or deficiency, in contrast to blood levels, which unfortunately fluctuate considerably under various medical situations, particularly with infections. Following are some interactions of iron and manganese with other elements:

There is also a synergistic and antagonistic interaction between Iron + Manganese and B-Vitamins, whereby these interactions will change under various medical situations as well. For instances, with kidney disease, a fine balance needs to be maintained between folate and iron levels since one will otherwise inhibit the other. The same applies with adrenal disturbances, except they will affect the balance between iron and Vitamin B1.

Stomach acid levels heavily interact synergistically with iron and manganese, whereby the absorption of both elements is enhanced by higher HCl acid levels, while an increase in iron or manganese will generally, but not always, result in raised stomach acid levels. Since Calcium and Magnesium have the exact opposite effect on stomach acid levels, their interaction with iron and manganese have a major impact on medical situations that are associated with raised or lowered stomach acid levels (for details see "Calcium & Magnesium").
Liver Functions:
Excessive manganese and/or iron storage can set the stage for tumor development as much as 10 or 20 years before a benign or malignant growth develops - subsequent to the exposure or intake of substances that have an adverse effect on Liver Chemistry, which includes:

- Alcohol
- Green Tea extract
- Antifungal medications
- Acetaminophen (Tylenol)
- Viral infections (e.g. hepatitis)
- Cholesterol-lowering (statin) drugs
- Food-related mold / mycotoxins (aflatoxin)
- Proton pump inhibitors (Nexium, Prilosec, Prevacid...)
- Hormones (e.g. estrogen, androgen, anabolic steroids)
- Heavy metal / toxic exposure (PVC, arsenic, pesticides)
- Dry cleaning chemicals (tetrachloroethylene / perchloroethylene)
- Genetic disposition (alpha-1 antitrypsin deficiency, hemochromatosis)
- Foods / beverages heated in plasticware containing Bisphenol A (BPA)
- Herbal / nutritional supplements (Lakota, kava, devil's claw, celandine, comfrey, chaparral)
- Evening primrose oil (EPO) and Conjugated Linoleic Acid (CLA) impair liver functions in some individuals. Symptoms include mild, but chronic nausea
Many other factors or medications (certain antibiotics, anesthetics, tricyclic antidepressants, anti-hypertensive, antiviral, anti-seizure... drugs) can result in higher manganese (and some in excessive iron) storage, regardless of actual manganese or iron consumption. In addition, certain foods or beverages (grapefruit or grapefruit juice) can alter the liver's ability to metabolize many toxins and drugs, resulting in higher iron and/or manganese retention as well.
By the time a tumor develops, patients don't always exhibit liver storage of these elements any longer, or they may have dropped below normal as a result of perimenopausal or postmenopausal hormone changes, along with reduced stomach acid levels.
From many years of following patients with a similar medical history, it appears that if stomach acid levels and liver functions are normalized in time, patients remain largely tumor-free. That approach is also helpful after cancer has developed, where following successful therapy, cancer is more likely to stay in remission. High manganese levels are linked to estrogen receptor-positive, while low manganese levels are linked to estrogen receptor-negative cancers.
The primary function of Iron in the body is the formation of hemoglobin, the essential oxygen-carrying component of the red blood cell (RBC). In combination with protein, iron is carried in the blood to the bone marrow, where with the help of copper, it forms hemoglobin. Red blood cells pick up oxygen from the lungs and distribute it to the rest of the tissues, all of which need oxygen to survive. Iron absorbed into the blood is usually bound to the protein transferrin and goes mainly to the bone marrow, where it can be used to make red blood cells.
Myoglobin is a red, iron-containing protein, which stores oxygen for muscle contraction. There are about 3 mg to 5 gm of iron in the body, of which hemoglobin represents 65%, while about 30% occurs as ferritin, which is the iron storage complex found in the liver, spleen and bone marrow. Neutrophils (white blood cells) depend on iron to help generate superoxide to function as a bacteria-destroying agent, whereby inadequate iron levels reduce the effectiveness of the immune system. With severe iron deficiency, hemoglobin levels decline and the packed volume of red blood cells, the hematocrit, declines.

Heme Iron from meat is about 10 times more absorbable [1] than iron from all plant / vegetable sources. Many vegans have trouble obtaining sufficient iron from the diet alone since phytates present in whole grains and oxalates found in certain vegetables may bind to some of the iron and reduce absorption.
Iron deficiency is more common during infancy, childhood, adolescence, pregnancy, menstruation, chronic infections, low stomach acid (sometimes from low salt intake), chronic diarrhea, impaired absorption (celiac disease), or bleeding.
The elderly may become iron deficient due to inadequate dietary intake or poorer absorption of iron. Vitamin C, protein, niacinamide and sufficient stomach acid all help iron absorption.
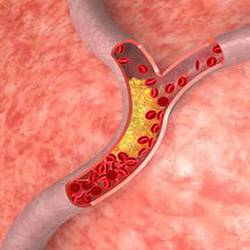
Iron Toxicity (high organ storage of iron) and/or high blood levels of iron are associated with an increased risk of free radical damage and cancer. Ferritin levels are a good indication of iron storage levels. Normal values for females range from 18 - 180 ng/ml (mcg/L), and 18 - 270 ng/ml for males. Levels below 15 ng/ml suggest very depleted iron reserves, and higher ferritin (> 350 ng/ml) can be a risk factor for cardiovascular disease and diabetes. Free radicals formed as a result of high iron can attack low-density lipoproteins (LDL) and subsequently lead to fatty plaque buildup, damage to the walls of arteries, as well as heart muscle tissue.
Iron supplements frequently cause constipation or stomach complaints, which may result from the use of ferrous sulfate, or similar hard-to-digest forms of iron. Other types of iron such as ferrous gluconate, ferrous fumarate, or ideally Chelated Iron Supplements are generally better tolerated, and there are also water-soluble iron products that are probably the least problematic on the body, and cause less of these effects.
Manganese is a much neglected, but important element when trying to stabilize blood sugar with diabetic and hypoglycemic individuals, and for lowering total cholesterol (cholesterol-lowering drugs frequently raise manganese levels).
It has strong estrogenic properties, and as a result is the most important element when nutritionally treating menopausal symptoms, menstrual problems, osteoporosis, and postpartum depression, for which manganese, along with Vitamin B1, is most effective. Manipulating manganese (or DHEA) levels can be an effective way to delay, or (sometimes) hasten menopause, trigger the menstrual cycle again after starting menopause, or along with iron and iodine levels, affect the frequency, duration and heaviness of the menstrual cycle.
Like iron, manganese can be helpful with some types of asthma, where lung capacity measurably improvers proportional to manganese intake. Extra supplementation of manganese may be helpful in some cases of carpal tunnel syndrome, deafness, epilepsy, infertility, and lack of libido in both sexes. In addition, individuals who regularly dislocate joints (particularly knee joints), frequently present with insufficient manganese levels, so normalizing manganese in those cases will permanently resolve that problem. On the other hand, high manganese levels increase the risk for tendon / ligament tears.
Manganese is important to many enzyme systems such as protein metabolism, bone formation, and the synthesis of L-dopamine and cholesterol, as well as carbohydrate metabolism, where it is required for the synthesis of glucose from non-carbohydrate substances (gluconeogenesis). As a co-factor in glycolysis, manganese aids glucose metabolism.
It is also needed for normal muscle and brain function,[2] blood clotting, and DNA and RNA synthesis, and it activates the enzyme responsible for the formation of urea. Manganese may help with some symptoms of Parkinson's disease such as muscle rigidity and twitching, although an excessive level of manganese can in itself produce Parkinsonian syndrome from a loss of dopamine in the brain cells. L-dopa, which converts to dopamine in the brain, is used in the treatment of manganese toxicity to reduce the symptoms.
High levels of manganese can produce violence and other mental changes, including a psychiatric disorder resembling schizophrenia.
When people supplement certain herbs to "cleanse" their liver, they will always affect manganese and iron status. For instance, by taking Devil's Claw on an ongoing basis, they will eventually raise manganese and iron levels. On the other hand, taking higher amounts of Milk Thistle will in time decrease manganese and iron stores, which can be an advantage with hemochromatosis (excess iron storage disease), where regular consumption of milk thistle, RNA / DNA, zinc, magnesium and Vitamin B2 - as individually matched - will return iron levels closer to normal, and frequently eliminate the need for phlebotomies.
 Manganese may help with some symptoms of Parkinson's disease such as muscle rigidity and twitching...
Manganese may help with some symptoms of Parkinson's disease such as muscle rigidity and twitching...
 Research shows that phytosterols such as beta-sitosterol may help normalize the function of natural killer cells and T-helper lymphocytes...
Research shows that phytosterols such as beta-sitosterol may help normalize the function of natural killer cells and T-helper lymphocytes...
 Iron deficiency may be suspect with some forms of ADHD. 84% of children with ADHD were found to have abnormally low levels of ferritin...
Iron deficiency may be suspect with some forms of ADHD. 84% of children with ADHD were found to have abnormally low levels of ferritin...
 A high intake of B Vitamins can trigger heart palpitations, HBP, major complications in patients with congestive heart disease...
A high intake of B Vitamins can trigger heart palpitations, HBP, major complications in patients with congestive heart disease...