Phosphorus and Sodium
| Cellular Nutrition
Phosphorus (P) and Sodium (Na) are associated minerals, and considered essential to human health. When using intracellular measurements, phosphorus and sodium allow for unique diagnostic and therapeutic properties regarding renal functions, where in contrast to their serum status, cellular levels extend from a low degenerative, to a high inflammatory range. Both kidneys are capable of handling the entire range of renal functions, but the right kidney tends to control sodium-related aspects, and the left kidney protein / phosphorus-related aspects, provided both kidneys are present, and in reasonable health.
While this may initially sound strange to some uninformed practitioners, it makes a lot of sense once the reasons are analyzed why in a high percentage of cases, patients end up with only one-sided kidney disturbances, whether they be infections, kidney stones, or other problems.
It is not unusual to hear of patients who produce hundreds, or even thousands of kidney stones in one kidney only, but never the other, unless the first involved kidney is removed.
When comparing the chemical profiles of a kidney donor and the kidney recipient before and after surgery, one gains a wealth of information on individual kidney functions and how to assist in their efficiency without drugs, and how they are not equal in maintaining pH balance, which can be very easily measured in both, the donor and recipient, after either the left or right kidney is donated.
For instance, when a patient presents with a Urinary Tract Infection (UTI), a cellular analysis will reveal the involvement and extent of the condition:
- If the bladder is affected, there is a significant rise in potassium.
- If the right kidney is affected, there is a significant rise in sodium.
- If the left kidney is affected, there is a significant rise in phosphorus.
Treatments can be formulated accordingly - either by prescribing conventional medications (if not familiar with nutritional concepts), or by simply lowering elevated levels pertaining to the above indicators, using common nutritional or biochemical principles:
| Sodium: | Vitamin B2, chromium, magnesium, potassium, zinc, folate |
| Phosphorus: | Vitamin B5 (pantothenic acid), calcium, zinc |
| Potassium: | Vitamin B3/4, chromium, magnesium, manganese, sulfur |
Intracellular tests will identify the appropriate minerals / nutrients which will be low in ratio to the one(s) corresponding to the infection, and will thus help identify a (contributing) cause, provide a treatment, and establish a basis for future prevention. While potassium supplementation could be theoretically considered with right-sided kidney infections, it has to be used with caution because of its pro-inflammatory effect on the bladder when high, and in the event of a kidney and bladder infection, potassium would have to be lowered along with sodium.
When selectively overdosing on phosphorus / protein or sodium beyond an individual's renal capacity, and provided both kidneys are equally healthy at the start, the right kidney will become diseased first with sodium, and the left one first with phosphorus (or protein). Very one-sided diets, or long-term use of specific drugs can affect both kidneys differently as well.
Despite its essential requirement, sodium (salt) tends to suffer a bad reputation as a result of being linked to cardiovascular disease and stroke. While one cannot dispute its involvement, sodium only affects about one third of the population in that regard. The rest can be divided among those where:
- someone's health is largely unaffected by the amount of salt (sodium chloride) consumed,
- adequate sodium / salt intake is necessary to help counteract a tendency for low blood pressure and low sodium-related symptoms, such as dehydration, depression, fatigue, spinal / joint degeneration, muscle cramps..., as well as help reverse higher LDL / HDL cholesterol ratios. While the liver largely controls total cholesterol, kidney chemistry has a primary effect on LDL / HDL ratios, whereby low phosphorus and protein encourage a higher production of VLDL triglycerides, while low sodium encourages a higher production of LDL cholesterol.

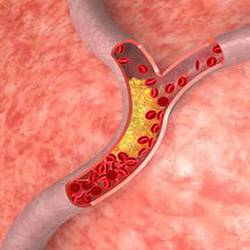
As a result, low sodium can actually increase the risk for heart disease, but reduces the risk for stroke, while high sodium, by reducing atherogenic development (arterial clogging), decreases the risk for some types of heart disease, however it dramatically raises the risk for stroke when potassium levels fall below those of sodium.
On the other hand, a high sodium / magnesium ratio, and/or a high phosphorus / calcium ratio are implicated with some forms of gout. Depending how efficient the body is in recycling chloride, low salt intake can also be a reason for reduced stomach acid levels.
In such a case, the strategy is not to increase someone's salt intake (which would otherwise cause more dehydration), but to boost aldosterone levels, which will subsequently increase sodium retention. Nutritional factors such as choline, licorice, iron, Vitamin B1, and - to a small extent - Vitamin E can be used for that purpose, which should be matched to individual requirements.
Occasionally Dr. Ronald Roth saw patients exhibiting very low sodium and medication-resistant high blood pressure, in which case sodium-raising supplements - by normalizing blood viscosity - resolve their hypertension.
Since an individual's Renal Capacity declines over a lifetime, it may be prudent for anyone - especially those with a family history of kidney problems - to avoid drugs, medications, or foods and nutritional supplements that have a tendency to compromise kidney functions and accelerate that process. Most prescription drugs, particularly blood thinners and NSAIDs, and many OTC drugs (Aspirin, Ibuprofen...) have a detrimental effect on renal functions, so patients and their practitioners have to carefully weigh a drug's benefits against those negative aspects.
Dietary factors that - in excess - have an unfavorable impact on kidney functions include foods with a high Oxalic Acid content [1] such as found in rhubarb, Swiss chard, spinach, parsley, cocoa products, and beets (especially beet greens), very high protein diets that are followed for longer periods of time, high phosphorus containing foods or beverages (meats, seafood, eggs, grains, dairy, nuts, soft drinks), excessive amounts of alcohol, creatine supplements, as well as real (glycyrrhizin-containing) licorice.
The same applies to insufficient intake of calcium, magnesium, potassium, zinc, Vitamin K, Vitamin C with bioflavonoids, Vitamin B2 (riboflavin), Vitamin B5 (pantothenic acid), and other essential nutrients. Of course a single, major kidney infection (e.g. from E. Coli) may cause enough kidney damage to result in early hypertension, or even require dialysis.

Foot odor is almost entirely related to kidney functions, and only to a lesser degree to tight, enclosed shoes. Similarly, Fungal Infections such as Athlete's Foot (tinea pedis), can only take place when the "terrain" allows the spread of a fungus - with the terrain being determined by the chemical make-up of the foot sweat of people with reduced or impaired kidney functions.
Anyone with healthy kidneys can walk across a wet gym floor and will not end up with athlete's foot. Normalizing renal chemistry (i.e. sodium, protein / phosphates) will normalize the chemical composition of someone's foot sweat, followed by the disappearance of any fungal infections, as well as foot odor.
Phosphorus, when high in ratio to calcium, is well established as being a contributing factor with osteopenia or osteoporosis, and many articles have been published on the risks of consuming too many soft drinks due to their high phosphorus content. A similar message is being preached regarding protein, supposedly having the same effect on calcium loss. Forgetting about the hype or agenda for a moment, any viewpoint can be correct for specific individuals, but it cannot be applied for everyone, as there are as many people who exhibit below-normal protein / phosphates, as are those who are above-normal, so only individual assessments are valid.
Osteoporosis and arthritic complaints can develop with high and low protein / phosphate levels, which subsequently rules out any "one-size-fits-all"- types of recommendations.
Long-term monitoring of patients shows high / low sodium-related cases being more right-sided in regard to joint damage, while high / low protein + phosphate-related cases are generally more left-sided in regard to joint damage, so striking a happy medium goes a long way in the prevention of many of these problems.
Phosphorus and calcium metabolism is linked, and requires Vitamin D for adequate uptake. Blood levels of phosphorus are increased by parathyroid hormone, and decreased by the thyroid hormone calcitonin. The kidneys excrete phosphates if blood levels rise, and they excrete less when dietary phosphate intake is low.
Phosphorus is present as Phytates in grains and cereals, so if bread is made from unleavened flour, the phytic acid will bind to iron, calcium, zinc and other minerals and reduce their rate of absorption.
Phosphorus aids muscle contraction, acts as a buffer for acid-base balance in the body, helps regulate the heartbeat, and supports proper nerve conduction. It is also necessary for the conversion of niacin and riboflavin to their active coenzyme forms.
Hormonal control of sodium (as well as chloride and potassium) balance is regulated by the adrenal cortex hormones as well as by the anterior pituitary gland. Addison's Disease is a life-threatening disease [2] caused by partial or complete failure of the adrenal cortex and involves the loss of sodium and potassium. Symptoms include weakness, muscle cramps, loss of appetite, weight loss, cold sensitivity, and salt craving.
Other sodium deficiencies can result from heavy sweating, or with severe dietary restriction, i.e. low sodium formulas fed to infants caused their brains to swell, causing death. Sodium plays a vital role in controlling osmotic pressure, which develops between the blood and cells due to ionic concentration differences, and it assists in maintaining the proper acid-base balance by balancing charges of negatively charged ions such as chloride, phosphate and bicarbonate.
The total volume of extracellular fluid is determined by sodium levels, while sodium concentration and water balance are controlled by the interplay of the kidneys and a number of hormones. When the level of sodium drops, the kidney releases the enzyme renin.
Renin catalyzes the conversion of a blood protein to angiotensin, which in turn stimulates the adrenal gland to release aldosterone, a hormone that causes the kidney to increase the rate of sodium reabsorption to correct the original sodium depletion. When dietary sodium intake is high, the kidneys rapidly excretes sodium, but its retention can lead to edema / water retention.
 Manganese may help with some symptoms of Parkinson's disease such as muscle rigidity and twitching...
Manganese may help with some symptoms of Parkinson's disease such as muscle rigidity and twitching...
 Research shows that phytosterols such as beta-sitosterol may help normalize the function of natural killer cells and T-helper lymphocytes...
Research shows that phytosterols such as beta-sitosterol may help normalize the function of natural killer cells and T-helper lymphocytes...
 Iron deficiency may be suspect with some forms of ADHD. 84% of children with ADHD were found to have abnormally low levels of ferritin...
Iron deficiency may be suspect with some forms of ADHD. 84% of children with ADHD were found to have abnormally low levels of ferritin...
 A high intake of B Vitamins can trigger heart palpitations, HBP, major complications in patients with congestive heart disease...
A high intake of B Vitamins can trigger heart palpitations, HBP, major complications in patients with congestive heart disease...